What Is Prostate Cancer?
Prostate cancer is the development of cancer cells in the prostate gland. (The prostate gland produces fluid for semen). It is the most common cancer in men; some cases of prostate cancers grow very slowly, while others are very aggressive and spread quickly to other organs.
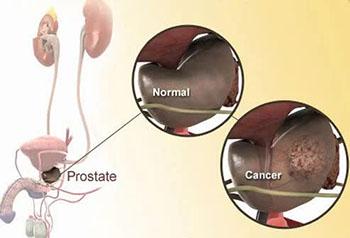
How Does Prostate Cancer Develop?
Like all cancers, prostate cancer begins when a mass of cells has grown out of control and begins invading other tissues. Cells become cancerous due to the accumulation of defects, or mutations, in their DNA.
Most of the time, cells are able to detect and repair DNA damage. If a cell is severely damaged and cannot repair itself, it undergoes so-called programmed cell death or apoptosis. Cancer occurs when damaged cells grow, divide, and spread abnormally instead of self-destructing as they should.
Prostate Cancer Symptoms
Symptoms of prostate cancer are variable; some men have no symptoms until the cancer develops over years. However, symptoms that can develop include the following:
- Urinary frequency
- Difficulty starting or stopping urination
- Interrupted or weak or slow urinary stream
- Blood in urine or in semen
- Discomfort (pain or burning sensation with urination or ejaculation)
- Intense pain in the low back, hips, or thighs, often present with aggressive or prostatic cancer spread to other organs
Prostate Cancer or Enlarged Prostate?
Two conditions can cause some symptoms that mimic those seen in prostate cancer described previously.
Benign prostatic hyperplasia (BPH)
BPH results from the prostate growing larger. BPH causes symptoms by creating pressure on the bladder, urethra, or both. BPH commonly occurs in elderly men and is a relatively benign condition.
Prostatitis (inflammation or infection of the prostate gland)
In the case of prostatitis, prostate tissue becomes inflamed, causing the prostate gland to swell. Any bacteria that can cause a urinary tract infection (UTI) can also cause prostatitis, and it may be caused by sexually transmitted diseases (STDs) including chlamydia and gonorrhea.
Both conditions are treated medically but some individuals with BPH may require surgical treatment.
Prostate cancer is differentiated from the above conditions by identifying cancer cells in a biopsy of the prostate.
Who Is at Risk of Prostate Cancer?
Aging in men (beginning at age 50) is the greatest risk factor for both BPH and prostate cancer. In addition, having a father or brother with prostate cancer doubles the risk for prostate cancer; however, African American males have the highest risk for prostate cancer. Research suggests that the majority of men at age 70 have some form of prostatic cancer with most of them showing no symptoms.
Preventing Prostate Cance
Researchers suggest a diet low in fruits and vegetables but high in meats and high-fat dairy products increases the risk for prostate cancer. The mechanism(s) for this is being investigated, but current speculation suggests meat and high-fat foods contain compounds that augment the growth of cancer cells. Exercise may also reduce your risk.
Can Too Much Sex Cause Prostate Cancer?
There are many myths about why prostate cancer develops. However, there is no evidence that “too much sex,” masturbation, benign prostatic hyperplasia (BPH), or a vasectomy increases the risk or causes prostate cancer. Current research is investigating if STDs, prostatitis, or alcohol use increase the risk of developing prostate cancer.
Prostate Cancer Screening Guidelines
Although screening tests are not routinely done for prostatic cancers, the American Cancer Society guidelines suggest some men should be screened.
Screening Guidelines Based on Age and Risk
- Men aged 40 with more than one close relative (father, brother, or son) diagnosed with prostate cancer at an early age
- Men aged 45 that are African American or have a father, brother, or son diagnosed with prostate cancer before age 65
- Men aged 50 or older who have average risk and expect to live at least 10 more years
However, not everyone agrees with these guidelines; clinicians should explain that treatments can have severe side effects, may have little or no effects on the cancer, and that some cancers are so slow-growing.
Digital Rectal Exam and PSA Test
Two tests are particularly helpful in screening for prostate cancer.
Digital rectal exam (DRE)
A DRE is done to determine if the prostate is enlarged and is either soft, has bumps or is very firm (hard prostate). During a digital rectal exam, a doctor checks for prostate abnormalities using a gloved, lubricated finger (digit).
PSA Test
Another test is done on a blood sample to determine the level of a protein (prostate-specific antigen or PSA) produced by prostate cells. The PSA test may indicate a person has a higher chance of having prostate cancer but controversies about the test exist (see following slide). The patient and his doctor need to carefully consider the meaning and the use of these test results.
PSA Test Results
In general, a PSA level less than 4 nanograms per milliliter (ng/mL) of blood is considered a normal level while a PSA greater than 10 ng/mL suggests a high risk of having cancer. Unfortunately, some men have intermediate levels (5 to 9 ng/mL), making their situations more difficult to judge. To make matters worse, some men have prostate cancer despite showing PSA levels of less than 4 ng.
PSA Test False Positives
BPH and prostatitis can increase PSA levels resulting in a false positive test.
PSA Test False Negatives
Some drugs may lower PSA levels and result in a false negative PSA test. Your doctor can help decide the meaning of both the PSA test and the digital rectal exam results and determine if additional tests need to be done.
Prostate Cancer Biopsy
If your doctor determines that the PSA and digital rectal exam suggest prostate cancer, the physician may suggest that a biopsy of the prostate is warranted, depending on your age, medical condition, and other factors. A biopsy is done by inserting a needle through the rectum or between the rectum and scrotal junction and then removing small samples of prostatic tissue that can be examined under a microscope for cancer tissue. The biopsy may detect and determine the aggressiveness of prostatic cancer cells.
Prostate Cancer Gleason Score
Biopsy samples from the prostate gland are examined by a pathologist. The pathologist makes determinations based on the samples as to the aggressiveness of the cancer. This determination is called the Gleason score.
How the Gleason Score Is Determined
The pathologist gives the prostate biopsy tissue a grade of 1 to 5, with 5 as the worst grade of tumor pattern. Then the pathologist looks at the individual cells in the tumor pattern and grades the cell types from 1 to 5 with 5 being the most aggressive cancer cell type. The Gleason score is based on the sum of these two numbers (tissue grade and cell type grade). A Gleason score of 5 + 5 = 10 indicates a highly aggressive prostate tumor while a low score (2 + 2 = 4) indicates a less aggressive cancer.
Prostate Cancer Imaging
The spread of prostate cancer may be detected by several different tests such as ultrasound, CT, MRI, and a radionuclide bone scan. Doctors will help determine which tests are best for each individual patient.
Prostate Cancer Staging
Prostate cancer staging is a method that indicates how far the cancer has spread in the body and is used to help determine the best treatment method for the patient. Cancer that has spread to other body sites or organs is termed metastatic cancer.
The Stages of Prostate Cancer
In terms of prostate cancer, the cancer stages are as follows:
- Stage I: The cancer is small and still contained within the prostate gland.
- Stage II: The cancer is more advanced, but is still confined within the prostate gland.
- Stage III: The cancer has spread to the outer part of the prostate and to the nearby seminal vesicles.
- Stage IV: The cancer has spread to lymph nodes, other nearby organs, or tissues such as the rectum or bladder, or to distant sites such as the lungs or bones.
- Aggressive prostate cancer often reaches stage IV but others that are less aggressive may never progress past stage I, II, or III.
Prostate Cancer Survival Rates
In most individuals, prostate cancer progresses slowly through stages; about all individuals diagnosed with stage I through III prostate cancer survive 5 years or longer and with current treatments, the outlook is even better for future survival.
Stage 4 Prostate Cancer
Even stage IV has a 5-year survival rate of about 31% and this figure may also increase with advancement in treatment methods.
Prostate Cancer Treatment: Watch and Wai
“Watch and wait,” is a phrase that is being used more frequently to describe a program of active surveillance without other cancer treatment for some patients with prostate cancer. It means that if your cancer is not aggressive (based on the Gleason score and the cancer stage), treatments may be deferred and your condition periodically checked. This approach is used because the risks of urinary and sexual problems inherent in most prostate cancer treatments are serious and may be put off or avoided if the cancer is not aggressive. However, aggressive prostatic cancer is usually treated even if secondary complications of treatments are serious.
Prostate Cancer Treatment: Radiation Therapy
Radiation, focused as a beam, can be used to kill cancer cells, especially those cells that have migrated (metastasized) from the prostate gland. Beams of radiation can be used to reduce bone pain caused by invasive cancer cells.
Low Dose Rate Brachytherapy
In another type of radiation therapy termed low dose rate brachytherapy, radioactive pellets about the size of a grain of rice are inserted into the prostate.
High Dose Rate Brachytherapy
High dose rate brachytherapy applies more radioactive sources temporarily into the cancerous prostate gland.
Both methods have side effects that can include erectile dysfunction, urinary tract problems, diarrhea, and other side effects.
Prostate Cancer Treatment: Prostate Cancer Surgery
Radical prostatectomy is the surgical removal of the prostate gland. Usually, this treatment is performed when the cancer is located only in the prostate gland. New surgical techniques help avoid damage to nerves, but the surgery may still have the side effects of erectile dysfunction and impaired urinary control. However, these side effects may gradually improve in some patients. Surgeons today may use robotic technique to assist in the operation.
Tips: Coping With Incontinence
Urinary incontinence is a common complication for men following prostate cancer surgery, and this problem can persist even five years after the surgery takes place. In one survey of 111 men published in 2003, 69% reported incontinence after prostate surgery. Most of these men used pelvic muscle exercises (Kegel exercises) to help. Many used containment devices, including pads, special underwear, and sanitary napkins to manage incontinence.
Here are some post-surgical incontinence tips:
- Keep a diary of how much you drink, and when and how often you use the bathroom. Note when you leak, and consider whether something could have caused the leak, such as bending in a certain way or drinking too much coffee or soda. The diary can give your doctor powerful in formation to help further your treatment.
- Practice double-voiding, meaning that after you finish urinating, wait a minute and try again.
- Drink less caffeine and alcohol. Both of these drugs can irritate the bladder and increase your need to go. Reducing or eliminating them from your diet can help stave off the frequent need to urinate.
- Avoid food triggers that for some men include chocolates, artificial sweeteners, spicy, or acidic foods. Other men find that food plays a small role or no role at all in their incontinence problems.
- Quit smoking. Along with all of its other many health hazards, tobacco has been linked with aggravated urinary incontinence in men.
Medicine Net